The interest in swimming continues to grow, both as an exercise program and a competitive sport. In 1995, Stocker, et al., reported that 100 million Americans classified themselves as swimmers.1 The participation of so many young people in competitive swimming leagues is an encouraging trend for a generation considered lacking in physical fitness. Swimming provides continuous dynamic activity to a number of large muscle groups, avoids the shock-stress-factors of other weightbearing athletic activities, and builds cardiovascular endurance.
However, the dedication of some swimmers to achieve more laps per workout or faster times may pose a hazard to musculoskeletal health. In particular, over 50 percent of the participants in the Stocker, et al., study - competitive collegiate swimmers and an older, less elite group, both of which experienced shoulder pain - perceived that increased intensities or distance provoked shoulder pain, indicating that fatigue may be the issue to avoid and on which to focus.1 Rovere also reported an increase in the incidence of overuse syndrome injuries among competitive swimmers.2 Many of these cases can be termed "swimmer's shoulder," referring to the many symptoms that develop in response to repeated, excessive overhead motions of the shoulder complex.3 In younger athletes involved in such motions, Jobe and Pink asserted that musculoskeletal instability is at the core of most shoulder injuries.4
Professionals who coach or train swimmers can help reverse this trend by placing more emphasis on prevention. Educating swimmers on the nature of fatigue associated with shoulder overuse, and encouraging regular use of strengthening exercises, can help make the sport more enjoyable for recreational swimmers and more successful for competitors.
Therapeutic exercise also is beneficial in the treatment of shoulder injuries. A prescribed rehabilitation program, carried out under regular supervision, has been shown to speed recovery and return to activity; increase muscular strength and flexibility; and prevent reinjury.4,5
Anatomic Review
A brief anatomic overview of the shoulder girdle is helpful in understanding the role of exercise in conditioning for swimmers (and many other patients). Indeed, shoulder pain and shoulder impingement syndrome rank with headache and backache as leading complaints seen by clinicians.6
Three bones, seven joints and three muscle groups provide form and function in the shoulder, regarded as one of the body's most mobile structures.6 Its wide-ranging mobility is sustained by a dynamic stability that requires near-perfect coordination and balance among connective tissues and muscles.
The primary muscles involved in shoulder movement are the deltoid, latissimus dorsi and pectoralis major. Shoulder stability is provided by the rotator cuff muscles: supraspinatus, infraspinatus, teres minor and subscapularis (also called the SITS muscles).
An intricate interplay between the rotator cuff and deltoid muscle occurs as the arm is raised, controlling the head of the humerus to provide for normal mobility. The deltoid muscle pulls the humerus upward as the SITS muscles synchronously pull and rotate the bone to prevent impingement with the overlying acromial arch. The glenohumeral joint movement occurs as a gliding motion with a constantly changing rotational axis of rotation, not around a fixed axis. This requires the muscles to perform double-duty: motion and stabilization.7
Impingement of the rotator cuff tendons under the acromial arch, or abnormalities in the scapular rotator muscles, are believed to be primary pathologies in swimmer's shoulder.8,9 Microtrauma breakdown of involved tissues cannot be overcome, due to the amount of external stress (continued swimming) or a deficiency in the body's repair capacity (from aging or nutritional deficiency).
Swimming Motions
The motions of swimming involve maximum propulsive force applied over extremes of motion in the upper extremity. Frequently, shoulder syndromes are associated with the freestyle and butterfly strokes, which exhibit similar functional patterns.8
These strokes can be divided into two stages, each with three phases:
Pull-through stage; 65 percent to 70 percent of stroke.
hand entry
middle pull-through
end of pull-through
Recovery stage; 30 percent to 35 percent of stroke.
elbow lift
mid-recovery
hand entry
Electromyographic studies on land and in water have revealed how shoulder musculature performs at each stage.8
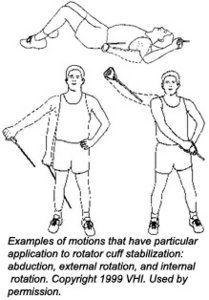
The SITS muscles are most active during the recovery stage, as the elbow is raised and the shoulder is abducted and externally rotated. Predominant activity in pull-through is performed by the latissimus dorsi and pectoralis major.
Most swimmers use the freestyle stroke for recreational or training workouts. The resistance generated in the pull-through stage creates hypertrophy of involved muscles and a comparative weakness in the recovery-stage muscles, leading to muscular imbalance or functional instability. Another biomechanical abnormality observed in swimmers is force-couple imbalance between internal and external rotators of the rotator cuff musculature.10 In either case, the stage is set for microtrauma breakdown.
Overcoming Instability
As noted previously, prevention is the best antidote to overuse syndromes, including swimmer's shoulder. Any coach or doctor who has required a dedicated athlete to suspend training or drop out of a competitive season while an injury heals can attest to the importance of avoiding injury.
A therapeutic exercise program is beneficial in preventing overuse syndromes when activities address specific musculature. To combat impingement and other manifestations of swimmer's shoulder, emphasis should be on functional stability with rotator cuff stability. Increased strength allows for greater control and stability to facilitate pain-free mobility.
With repetitive-motion injuries, there is the risk of developing selected muscles while acquiring a disuse atrophy in others. This may set the stage for an overuse injury. Restoring muscle balance in all ranges of motion may decrease the likelihood of injuries.
In rehabilitation of injured muscle, normal adhesion formation can be controlled through exercise, encouraging formation of a flexible scar. Other benefits include improved neuromuscular coordination, biomechanical efficiency, and reduction of atrophy and deconditioning.
A rehabilitation program utilizing high-grade surgical rubber tubing isolates activity to specific joints and musculature. The system incorporates eight basic isotonic exercise patterns, and patients progress in activity according to individual capabilities.
This type of rehabilitation system offers the added benefit of enabling a swimmer to exercise even when pain is present on abduction. The variable resistance afforded by the surgical tubing adapts to a range of strength abilities. Even minimal motion can be beneficial, due to a 15- degree physiologic overflow on each side of the exercised area.
References
Stocker D, Pink M, Jobe FW. Comparison of shoulder injury in collegiate- and master's-level swimmers. Clin J Sport Med 1995;5(1):4-8.
Rovere GE, Nichols, AW. Frequency, associated factors, treatment of breaststroker's knee in competitive swimmers. Am J Spts Med 1985;13(2):99-104.
Pink MM, Tibone JE. The painful shoulder in the swimming athlete. Orthop Clin North Am 2000;31(2):247-261.
Jobe FW, Pink M. Classification and treatment of shoulder dysfunction in the overhead athlete. J Orthop Sports Phys Ther 1993(Aug);18(2):427-432.
Roy S, Irvin R. Sports Medicine Prevention, Evaluation, Management, and Rehabilitation. Englewood Cliffs, Prentice-Hall, 1983.
Leahy PM, Mock LE. Altered biomechanics of shoulder and subscapularis. Chiro Spts Med 1991;5(3):62-66.
Nuber GE, et al. Fine wire electromyography analysis of muscles of shoulder during swimming. Am J Spts Med 1986;14(1):7-11.
Wadsworth DJ, Bullock-Saxton JE. Recruitment patterns of the scapular rotator muscles in freestyle swimmers with subacromial impingement. Int J Sports Med 1997(Nov);18(8):618-24.
Roodman WU. Etiologies of shoulder impingement syndrome in competitive swimmers. Chiro Spts Med 1989;3(2):27-31.
Kim Christensen, DC, DACRB, CCSP, CSCS Ridgefield, Washington
Spearheaded by burgeoning scientific and clinical research literature, psychedelics have reached a level of media coverage and popular interest that has not been seen for over half a century. By “psychedelics,” we are referring to the unique class of substances that includes psilocybin (the active compound found in so-called “magic mushrooms”), LSD, dimethyltryptamine (DMT), ayahuasca, 5-MeO-DMT, and mescaline – each of which occurs in the natural world (except for LSD, which is a semi-synthetic compound).
At its March 11, 2024, meeting, the Council for Higher Education Accreditation (CHEA) Committee on Recognition reviewed the formal request for a change in the CHEA-recognized scope of accreditation submitted by the Council on Chiropractic Education (CCE). The new CHEA-approved scope statement is: “The Council on Chiropractic Education accredits doctor of chiropractic degree programs and chiropractic residency programs in the United States, its territories and Canada (2024).”
Many relevant diagnostic signs are not performed deliberately by the examiner or by the patient at the examiner’s direction. They are observed as the patient reacts to their condition. Fortin’s finger sign, Minor’s sign, and Vanzetti’s sign are three examples of this principle.